
From thefaceofncds.org
A pandemic is sweeping the globe and has transpired into the world’s biggest killer. (And no it is not Ebola, however deadly it is proving to be.) They are killing millions every year. They are non-communicable diseases or NCDs; the five most common being cardiovascular disease, diabetes, cancer, chronic respiratory diseases and mental illness. While many are afraid that the Ebola epidemic will escalate by rapid transmission between individuals, NCDs are far more destructive despite not being transmissible, killing 35 million people worldwide annually; that is 60% of total global deaths. Many would stereotype the typical NCD patient as being an old, overweight lazy male in the Western world. The reality is very different, 80% of global NCD deaths occur in low- and middle- income countries, and 8 million of these people die below the age of 60. NCDs are fast becoming indicative of poverty, and a major burden on global health and development. So as young people who are passionate about tackling NCDs, is there anything we can do to stem the tide? Thankfully there is, and the NCDFREE bootcamp held in London a couple of weeks ago aimed to equip young people with the skills to make that change. We began with Prof. Richard Smith who asked if slavery can be abolished, why can’t NCDs? A strong social movement, like the abolitionists or the civil rights movement, is required. An element of outrage needs to be instilled in the public for meaningful change, resembling the outrage observed in relation to AIDS in the 1980s and climate change today. A multi-disciplinary team with a variety of skills to offer can produce a powerful movement and relay the message to lay people. Katie Dain of the NCD Alliance described the prevalence of facilities to support patients of infectious diseases in the developing world, but scarce support exists for NCD patients. She mentioned one diabetes patient who stated that he would rather have HIV, due to the lack of support he receives to manage his diabetes. Dain concluded that we in the Western world created this problem through globalisation and allowing the food industry to run riot. Now it’s time for us to solve it. Futerra co-founder, Ed Gillespie described the bystander effect – people hope someone else will solve the problem. Gillespie said we must understand that solving one problem can create another, but it is still a sign of progress we must persevere with. Jo Creed from the Jamie Oliver Food Foundation gave us a whirlwind tour of good and bad campaigns, ranging from personalised Coca Cola bottles to the no make-up selfie and the ice bucket challenge. A clear, simple and positive message proves most effective but the educational content is extremely important, as often people become involved in campaigns to gain attention rather than heeding the message. For example many who participated in the recent ice bucket challenge failed to either raise awareness of the rare neurodegenerative disorder amytrophic lateral sclerosis (ALS) or donate to the charity running the campaign. Dan Lewis-Toakley of the petition website Avaaz, emphasised the need to involve everyone to maximise a campaign’s impact. We must make use of powerful statistics but also use human stories; showing your own vulnerabilities can trigger emotional responses from your audience. Dr Corinna Hawkes from the World Cancer Research Fund gave a fascinating talk on how hidden political interests can often hinder progress in public health affairs. Once a high level UN meeting involved a heated debate on salted anchovies! It emerged that Nordic and Mediterranean countries were competing to promote their diets as being the ‘healthiest’ to increase business for their food products. To overcome this issue we must learn what political interests are at play, leverage them to our own interests, and learn to communicate with politicians or economists in their language, not in scientific terms they will not understand. We had an insight into social innovation from Dr Harpreet Sood, a Senior Fellow at NHS England, and Dr Fred Hersch, a Clinical Research Fellow at the George Institute for Global Health, Oxford. It is vital to have a strong multi-disciplinary team working on a specific aim within a reasonable time frame. But you will not know if your invention will be effective until you go out and test your prototype, so be open-minded and prepared to improve your product. The most moving account of the weekend came from filmmaker Batsheva Lazarus. She described how telling an individual’s story is often more persuasive than presenting a plethora of facts. As a scientist this was really eye-opening, we are trained to support every claim with experimental evidence, yet if you want to relay your message to the public or policymakers, they will simply get bored of listening to you. Introducing an emotional component by telling the story of someone who may be suffering from cancer in a low income country for example, can really help your message hit home. This is perhaps the magic behind the short advocacy films created by NCDFREE in Mongolia and Ghana, which have been shown to the WHO and included in global health courses. The final talk was from NCDFREE founder Dr Alessandro Demaio, a Global Health Fellow at Harvard Medical School, who spoke about his experiences as a leader. To be a successful leader of a movement like NCDFREE, you must truly believe in your idea and speak about it passionately. Having a multi-disciplinary team is helpful with a clear and shared vision. Remain positive in spite of the challenges you face, focus on finding solutions not the problems, provide support to your teammates to continue achieving and keep evaluating your own performance. Also featured in the bootcamp was a quiz to test our knowledge on NCDs, during which we learnt Halle Berry and Tom Hanks are among those suffering from diabetes! We were trained to relax and control our emotions with a session of yoga and meditation. And we participated in a group challenge to design a campaign and a 60 second film concept answering a real challenge facing the NCD community; the winning pitch will be made into an actual campaign film. The challenge facing my team was to devise a campaign involving smartphones to get young people to care about a disease they may not get for another 30 years. And I am delighted to say we came up with the winning pitch! We designed a film concept where a healthy and unhealthy person were using their smartphones to chat with their ‘future self’ 30 years ahead, and thus saw the consequences of their lifestyles on their health. We concluded the pitch encouraging viewers to join the #ticktock campaign (emphasising that their time is running out if they don’t improve their health) and share their healthy actions on social media. Check out the video of our winning pitch here: http://www.youtube.com/watch?v=ORe9_6ZZ1AM and if this becomes the next viral campaign, remember you heard it here first! In the meantime NCDFREE has launched #theface of NCDs campaign encouraging people to share their stories of how NCDs have affected their lives, whether it’s affecting their own health or those they love, or observing the impact on local communities and work environments. Do you have an NCD story you would like to share? If so visit http://www.thefaceofncds.org, share your story and help change the face of NCDs. This piece was originally published on Imperial College's Global Health blog Cafe Communique. It can be viewed here: http://cafecommunique.org/component/easyblog/?view=entry&id=58&Itemid=290
0 Comments
Just six weeks before his death in 2008, American TV journalist Tim Russert underwent a cardiac stress test, as he was already known to have coronary artery disease. He exercised on a treadmill while his blood pressure and heart were monitored. Despite being overweight, hypertensive and having excess cholesterol, which were controlled by medication and lifestyle changes, Russert did not display any symptoms suggestive of imminent cardiac problems. Yet within two months, he died of a sudden cardiac arrest. How did doctors miss this impending cardiac event? It seems that the body’s defence mechanisms eluded existing medical technology. As you may have read before (Blog post: Blocked Pipework in Our Hearts), our arteries detect that a growing atherosclerotic plaque can reduce blood flow to the intended tissues, so the artery wall expands outwards in an attempt to maintain the diameter of the artery through which blood flows. This process is referred to as positive remodelling or ‘Glagov remodelling’, named after the late Professor Seymour Glagov who demonstrated this phenomenon. Standard angiography – where a dye is administered into the patient’s coronary arteries and X-ray imaging is used to visualise arterial blood flow – will only reveal significant blockages or narrowing of arteries. But if an artery has remodelled considerably to maintain blood flow, atherosclerotic plaques will not be detected in spite of how large they may be. In fact, up to 75% of ruptured atherosclerotic plaques, which have significantly reduced or blocked blood flow, exhibit positive remodelling [1]. Once the plaque reaches the ‘Glagovian’ limit of blocking 40% of the cross-sectional area of the artery, expansion can no longer occur so further plaque growth only serves to block blood flow, otherwise referred to as negative remodelling [2]. This is when arterial disease will be detected by angiography. As described previously, smooth muscle cells from the artery wall move into the developing plaque and create a layer on top full of smooth muscle cells and collagen produced by these cells, called the fibrous cap. When this cap becomes extremely thin and weak, due to proteins produced by macrophages (the main inflammatory cell) breaking it down, the cap ruptures and can trigger the appearance of a blood clot. If a blood clot does not appear, the ruptured cap will heal itself with the further production of collagen from the smooth muscle cells. The plaque may undergo several cycles of rupture and repair without any blood clots and subsequent symptoms appearing. And it is this process that determines the speed at which the transition from positive to negative remodelling occurs. If the plaque is permitted to grow with the gradual intrusion of lipids and inflammatory cells, the transition may take decades. However repeating cycles of rupture and repair will rapidly increase the rate at which the plaque grows, thus a seemingly harmless plaque can suddenly present a major threat within months or even weeks. This chain of events was most likely responsible for the sudden and unforeseen demise of Tim Russert. 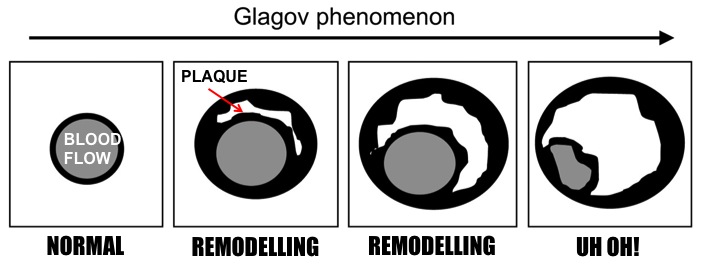 Remodelling of the Artery. Images adapted from Berman et al, (2006) Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Assessment of Patients with Suspected Coronary Artery Disease, J Nucl Med, 47(1): 74-82 So is there any hope of detecting these rapidly developing plaques before it is too late? Thanks to scientists like Professor Jagat Narula (whose recent lecture at Imperial College is the inspiration behind this blog post), there is now technology available to detect these invisible killers. Optical coherence tomography (OCT) imaging utilising near-infrared light, can be used to detect fibrous caps that are thinner than 65μm (μm = microns or micrometres, one thousandth of a millimetre), which are at high risk of rupturing. Computed tomography (CT) angiograms - where an iodine-rich dye is injected into the patient and then a CT scan of the blood vessels is performed – can be used to observe the necrotic core of plaques (full of dead or dying macrophages and lipids), which is linked to extensive remodelling of the artery, and the presence of calcium deposits in plaques; also indicative of an increased risk of clinical events [1]. This is an extremely important development as a higher degree of remodelling and larger necrotic cores are associated with an earlier onset of acute cardiovascular events. 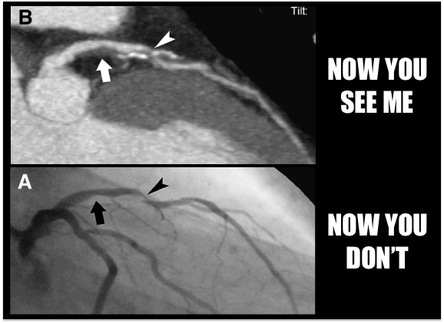 Top: CT image where two plaque are pointed out. The left-hand arrow shows a large plaque, right-hand arrow shows a calcified plaque (calcification in white). Bottom: Angiogram where blood flow appears in grey. Left-hand arrow shows the large plaque in the above image but blood flow is unaffected. Right-hand arrow shows blocked blood flow due to the calcified plaque. Images from Hoffmann et al, (2006) Coronary CT Angiography, J Nucl Med, 47(5): 797-806. It now appears that a combination of CT angiography, positron emission tomography (PET) and the use of FDG (if you really want to know what it stands for, it’s 2-fluorodeoxyglucose) as a contrast agent can be used to visualise plaques with a high level of macrophage-based inflammation [1]. As inflammatory cells have a high rate of metabolism, consuming larger amounts of glucose than other cells to generate energy for their demanding inflammatory activities, FDG acts like glucose and is taken up by these macrophages. And as the FDG is labelled with fluorine-18, a radioisotope emitting positrons as it decays, the PET scanner detects these positrons being emitted at a high rate within the plaque macrophages. Mannose is another sugar taken up by macrophages, and macrophages with the mannose receptor on their cell surface are more prevalent in high-risk plaques. Subsequently fluorine-18 labelled FDM (2-fluorodeoxymannose) has also been successfully used to image macrophage-based inflammation in atherosclerotic plaques [3]. In fact, macrophages take up a greater amount of FDM than FDG, especially when they are starved of oxygen (a condition called hypoxia) in the plaque, which has no direct blood supply until small leaky blood vessels grow into it later on. Thus FDM maybe a better option to image inflammatory plaques. While there is still work to do to improve the quality of these imaging methods and ease the discomfort for patients during the procedure, it is only matter of time until we can identify these dangerous high-risk plaques before it is too late. 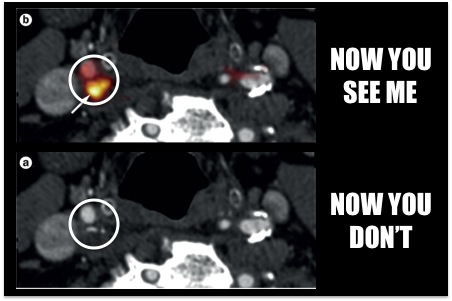 Top: PET-CT fused image where a plaque with inflammation is visible due to the 18F-FDG agent. Bottom: CT image without the use of 18F-FDG. You can't see the inflammation now! Images from Tarkin et al, (2014) PET imaging of inflammation in atherosclerosis, Nat Rev Cardiol, 11: 443-457. Atherosclerosis is broadly considered a disease of modern times caused by processed and fatty foods, low levels of exercise or old age. While these causes may apply to today’s patients, it is not a disease exclusive to current generations. CT scans of Egyptian, Peruvian, Native American and Russian mummies have detected calcified atherosclerosis in coronary arteries supplying blood to the heart, and carotid arteries supplying blood to the head, as is commonly seen in patients today [4]. But how could they possibly get atherosclerosis when their diets and lifestyles were completely different? Further examination of the mummies showed these individuals had black lungs, much like smokers of today. Thousands of years ago people relied on wood- or coal-fuelled fire for warmth and cooking, and were thus highly exposed to smoke and soot. Infectious diseases were also more prevalent, and high levels of chronic inflammation caused by infections are known to increase atherosclerosis. So as is commonly advised, don’t eat junk and don’t smoke. Not only will it keep your arteries clean, but do you really want to be the smelliest person on the train? I certainly won’t sit next to you….
References 1. Narula J, Nakano M, Virmani R, Kolodgie FD, Petersen R, Newcomb R, Malik S, Fuster V, Finn A V., Histopathologic characteristics of atherosclerotic coronary disease and implications of the findings for the invasive and noninvasive detection of vulnerable plaques., J. Am. Coll. Cardiol. 61 (10) (2013), 1041–51. 2. Finn A V, Nakano M, Narula J, Kolodgie FD, Virmani R., Concept of vulnerable/unstable plaque., Arterioscler. Thromb. Vasc. Biol. 30 (7) (2010), 1282–92. 3. Tahara N, Mukherjee J, Haas HJ de, Petrov AD, Tawakol A, Haider N, Tahara A, Constantinescu CC, Zhou J, Boersma HH, Imaizumi T, Nakano M, Finn A, Fayad Z, Virmani R, Fuster V, Bosca L, Narula J., 2-deoxy-2-[18F]fluoro-D-mannose positron emission tomography imaging in atherosclerosis., Nat. Med. 20 (2) (2014), 215–9. 4. Thompson RC, Allam AH, Lombardi GP, Wann LS, Sutherland ML, Sutherland JD, Soliman MA-T, Frohlich B, Mininberg DT, Monge JM, Vallodolid CM, Cox SL, Abd el-Maksoud G, Badr I, Miyamoto MI, el-Halim Nur el-Din A, Narula J, Finch CE, Thomas GS., Atherosclerosis across 4000 years of human history: the Horus study of four ancient populations., Lancet 381 (9873) (2013), 1211–22.  The majority of residents in England have benefited from free healthcare provided by the National Health Service (NHS). I think it is fair to say that the majority of us would be in a worse state of health or even not living if it wasn't for the NHS. The UK economy benefits by million of pounds every year as a result of the NHS keeping the British workforce healthy. According to the latest research, every £1 invested in public healthcare increases GDP by £3 [1]. Yet the government insists on cutting funding for the NHS, while it spends billions of taxpayers' money bailing out corrupt banks, maintaining the monarchy's lavish lifestyle, and fuelling futile wars overseas. Where is the sense in that?
I know how the NHS has helped me. I was born in an NHS hospital with no complications for me or my mother. As a baby my elbow was dislocated, and an NHS doctor popped it back in place. As a toddler I was hospitalised due to severe asthma, which thanks to the NHS is no longer a problem for me. My father was treated for a heart attack and had life-saving heart bypass surgery. Incredibly 10 years on, he is in excellent health. I have no idea how we could have possibly afforded to pay for his open heart surgery had the NHS not existed. And now I have the privilege of working with NHS doctors and scientists to hopefully find the next treatment for heart disease. Of course there are sometimes blunders, nothing is perfect but some healthcare is better than none at all. And the overwhelming majority of healthcare provided by the NHS is of the highest standard, arguably the best in the developed world [2]. If you have been relying on the BBC for your news, you will have no idea that we now face the possibility of no longer having access to free healthcare by the next general election, and blunders could become the norm with a privatised health service, prioritising profit over welfare. People from countries all over the world envy our national health service and yet our government is destroying it before our very eyes, just to gain lucrative business deals from their pals. If we don't act now, our NHS will disappear and we could pay with our lives, literally. After all good health is not a privilege, it is a human right. So think to yourself, how has the NHS helped you and could you live without it? Act now! Please join the ongoing People's March for the NHS, which will conclude with a rally in Trafalgar Square at 3.30pm on Saturday 6th September. Please visit 999callfornhs.org.uk for more details and sign up for the march! References [1] http://nhap.org/every-1-invested-public-healthcare-increases-gdp-3/ [2] http://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirror-mirror Re-organising the world's largest public health service could not only damage healthcare provision but also medical innovation  In March 2012, the Conservative and Liberal Democrat coalition government (also cynically known as the Con-Demned coalition) passed the Health and Social Care Act through parliament. The Act permits radical re-organisation of England’s world-renowned National Health Service (NHS). The scale of re-organisation, perhaps a misnomer for extensive privatisation, has raised serious concerns about the level of healthcare that will remain freely available to taxpayers. One concern that has not been discussed in great detail is how NHS privatisation will affect the future of medicine i.e. training future doctors and advancing medical innovation.
The Labour party founded the NHS in 1948, pledging to deliver high quality healthcare to all citizens regardless of wealth, and funded entirely by taxpayers [1]. The NHS has since expanded into the largest publicly funded health service in the world featuring world-renowned hospitals, and allowing patients to benefit from various health services they could not otherwise afford, ranging from dentists to open-heart surgery. As a result, the NHS is most beloved in the UK with consistently high levels of satisfaction expressed by patients. The majority of today’s population was born with the aid of NHS services, and many rely on state-funded healthcare during their lifetime. The UK’s life expectancy has also continued to rise since the NHS was founded. The UK was recently rated as having the best health service amongst 12 developed countries, including the US, Australia and Germany [2]. A vibrant health organisation placing skilled health professionals and scientists under one roof has fostered numerous medical discoveries, revolutionising healthcare not only within the NHS, but throughout the world. Examples include: the link between smoking and lung cancer, the UK’s first ever heart transplant, and the world’s first ‘test tube’ baby born as a result of in vitro fertilisation (IVF) [1]. So how will the re-organisation permitted by the Health and Social Act affect the ability of the NHS to deliver medical innovation? Squeezing of the NHS budget and increasing staff workloads in recent years already prompted a large migration of doctors to countries like Australia, in the hunt for reasonable salaries and a more manageable work-life balance. The loss of such valuable talent has harmed medical training and clinical research in the NHS. The transfer of services and facilities from the state to the private sector inevitably means profit is valued more than patient welfare. As a result we have already witnessed a multitude of hospital closures and staff redundancies, and this will aggravate existing problems. Unite the Union argues that the private sector may ‘cherry-pick’ more profitable services and surgical procedures causing a loss of low-demand but still vital services for some patients, and further opportunities to train junior doctors and medical students [3]. Most hospitals collaborate with academic research laboratories providing patient samples for research experiments. Hospital mergers and closures will drastically cut the number of collaborations and the pool of samples available for such research, thus limiting the rate at which progress can be made towards the next medical therapy. The private sector may even decide to charge for medical training and access to patient samples and clinical research facilities, elevating costs for medical students and researchers (generally funded by the taxpayer or charities) respectively. On the contrary, the government states that the private sector will play a greater role in medical research through an increase in academic-industry collaborations [4]. Such a move would be advantageous in obtaining funding for medical research, as private companies tend to offer more funding than research councils and charities. But naturally private investors will expect something in return. We are well aware that pharmaceutical companies have failed to invest in research on diseases plaguing developing counties, due to the lack of financial return [5]. Pharmaceutical companies often spend millions of pounds investing in the development of one drug, aiming to earn the money back from sales of the drug, which developing states cannot afford to pay for. Hence a similar trend could occur in the UK, where pharmaceutical and medical device companies may refuse to invest in research to develop treatments for rare diseases due to low prospects in profiting, or they may develop treatments but charge colossal amounts unaffordable for patients. With strengthening of academic-industry collaborations also comes the probability that more state and charity funding of academic research will result in discoveries that subsequently rely on industry to produce the treatment, and ultimately reap the profits. Of course these possibilities are hypothetical, but we have already seen evidence both within the NHS and in other scenarios that these negative consequences are unfolding and could severely jeopardise standards of healthcare delivery and the future of medical innovation, not only in the UK but worldwide. Are these consequences we want to live with? And in case you are wondering what is motivating this large-scale privatisation of the NHS, take a look at this: http://socialinvestigations.blogspot.co.uk/2012/02/nhs-privatisation-compilation-of.html Please join the People's March for the NHS, further details here: http://999callfornhs.org.uk Like what you read? Please vote for it by clicking on the + sign at The News Hub here: https://www.the-newshub.com/stories/why-the-nhs-is-vital-for-the-future-of-medicine References [1] http://www.nhs.uk/NHSEngland/thenhs/nhshistory/Pages/NHShistory1948.aspx [2] http://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirror-mirror [3] http://www.unitetheunion.org/uploaded/documents/GuideToNHSPrivatisation11-10734.pdf [4] https://www.gov.uk/government/publications/health-and-social-care-act-2012-fact-sheets [5] Book by Ben Goldacre (2012) Bad Pharma: How Medicine is Broken, and How We Can Fix It, Fourth Estate, UK.  Magazines and newspapers are full of so-called ‘tips’ or ‘advice’ for the image conscious, detailing extreme diets followed by the rich and famous to achieve dramatic weight loss, or new diets apparently supported by the latest scientific research. But how many of these fad diets are substantiated by scientific research? And are these diets safe to follow? Recently New Scientist featured an interesting discussion on the gluten-free diet, made fashionable particularly in the sporting world by current world number one tennis player Novak Djokovic [1]. Having developed a reputation for being physically weaker than his rivals, Djokovic was eventually diagnosed with coeliac disease and as being gluten-intolerant. Eliminating gluten from his diet transformed his career, he now often outlasts his opponents in gruelling matches and won six grand slam titles out of his career total of seven following the dietary change. Many have since adopted the gluten-free diet with the hope of boosting their energy levels, but have had mixed results. Recent studies show that being ‘gluten-intolerant’ is hardly a medical condition that can be diagnosed and scientists have struggled to establish a mechanism for supposed gluten intolerance. So unless you suffer from coeliac disease that is triggered by gluten, following a gluten-free diet could do more harm than good, as gluten-free foods are often low in fibre and key nutrients and high in sugar. The gluten-free diet is just one of many fad diets that benefit significantly from media hype. So to sort fact from fiction we need to ask for evidence. That is why scientific experts in the Voice of Young Science network (including myself) have teamed up to look for evidence behind over a dozen eccentric diets, promising to help you lose weight by keeping yourself cold, stop ageing by completely eliminating sugar, detox by eating clay and many more. What did we discover? Find out by visiting the Spoof Diets project webpage at: www.senseaboutscience.org/pages/spoof-diets.html. And just to keep you on your toes as the project name suggests, we’ve thrown in a few ‘spoof’ diets; can you spot them? You won’t believe the results!  You can follow more ‘Ask for Evidence’ projects involving the Voice of Young Science network on Twitter @voiceofyoungsci and by visiting the Sense About Science website [2]. In the meantime, enjoy figuring out which diets you should and should not follow, and remember always ask for evidence!
A recent study showed that a compound found in red meat called L-carnitine could be responsible for increasing the risk of vascular disease by altering the bacteria found in our guts [1]. Lets look at this study in further detail. L-carnitine and choline (found in excess amounts in eggs, dairy products) is broken down by our gut microbes into a compound called TMA, which is then converted by liver enzymes into TMAO - associated with cardiovascular disease and atherosclerosis. TMAO is detected in the blood of omnivores but not vegans, following the intake of L-carnitine capsules for three days. It seems a species of bacteria belonging to the genus Prevotella is the main bacterial population that metabolises carnitine into TMAO. And interesting point is that the presence of TMAO has no effect on the expression of the receptor for LDL (low density lipoproteins or bad cholesterol) or cholesterol production genes. So how can TMAO increase atherosclerosis? In the liver it prevents the breakdown of cholesterol into bile acids. It appears that TMAO also reduces a process called reverse cholesterol transport – the expulsion of excess cholesterol by gut cells, and macrophages in atherosclerotic plaques. TMAO does this by lowering the presence of cholesterol transporters in the gut. Thus if excess cholesterol cannot be eliminated from the circulation by gut cells, or the artery wall by macrophages, the development of atherosclerosis and the risk of cardiovascular disease increases. So now we know how red meat on its own can increase cardiovascular disease. Over the years it has been documented how the food industry handles red meat to enhance its visual appeal and marketability such as the use of red food colouring and soaking meat in salt water to enrich its flavour. We cannot establish on what scale such tampering has affected the health of the general population. But one thing is for certain, don’t eat meat that looks red. Reference [1] Koeth, R. a, Wang, Z., Levison, B. S., Buffa, J. a, Org, E., Sheehy, B. T., … Hazen, S. L. (2013). Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nature Medicine, 19, 576–85. doi:10.1038/nm.3145 You’ve heard all the usual health advice to keep your heart healthy or reduce your risk of cancer, but sometimes you are tempted by that mouth-watering piece of cake in the patisserie window or want to miss that workout for the day to catch your favourite TV show. And to be honest there is no harm in occasionally being a little lazy and treating yourself. But maybe you would find it easier to be healthy if you understand why taking such health precautions are good for you. In my previous post, you learned what causes heart attacks and strokes. Now here is how you can prevent them happening to you.  Fatty fatty! Fatty fatty! 1) Ditch the lard As mentioned in my previous post, fats are essential to start the atherosclerotic process. If there is too much ‘bad cholesterol’ (otherwise known as low density lipoproteins or LDL) and another type of fat call triglycerides, in your blood from all those hamburgers or a full English breakfast (red meat is particularly high in fat), they will deposit in curved or branching arteries triggering the immune response where macrophages initially consume the fats, clear them from the artery and break them down into cholesterol, which become a vital part of the cell membrane. However the amount of LDL eventually overwhelms macrophages, so they die and deposit in the artery wall contributing to the build up of the atherosclerotic plaque. And why in particular is LDL so dangerous? The clue is in the name, the particles are of a low density and thus are small enough to fit through the spaces between endothelial cells and deposit inside the artery wall, while also being more easily consumed by macrophages. The dying macrophages also contribute to the problem, as their cell membranes become part of the growing plaque increasing the level of cholesterol inside. And it’s not just the fat inside your arteries that creates problems. As more fat is consumed, the body primarily deposits the excess fat around the abdomen resulting in an increase in number and size of fat cells, called adipocytes, which are full of triglycerides and cholesterol. And crucially these adipocytes release chemicals, which increase the aggressive immune activity of macrophages, making them more likely to build up and cause damage in the artery wall. 2) Keep working out The recommended amount is equivalent to half an hour everyday, my suggestion is to do as much as you can! Research suggests that physical activity; particularly aerobic exercise (such as running, cycling, swimming) can lead to better control of the production of inflammatory signals, which would normally mobilise the immune cells, such as macrophages, responsible for exacerbating atherosclerosis. In fact exercise stimulates the production of anti-inflammatory signals, which dampen down the potentially damaging inflammation, reduce adipocytes, help macrophages to expel cholesterol, reduce growth of the plaque, and in already advanced plaques it can increase the thickness of the fibrous cap (by promoting the growth of smooth muscle cells) therefore it is less likely to rupture and create a blood clot. So it is never too late to start exercising, even as you get older it could save your life!  Don't you want to dive into that colourful fruit? Don't you want to dive into that colourful fruit? 3) Eat your five-a-day or even more! Studies show that the more fruit and vegetables you eat, the lower your risk of suffering a heart attack or stroke, particularly with green leafy vegetables and fruits such as apples. Research is ongoing to establish exactly why fruit and vegetables are so beneficial. Early studies suggest a protein called sulforaphane – found in green vegetables such as broccoli – can suppress the activation of endothelial cells, thus it could reduce atherosclerosis by preventing the chain of events that start the disease process. Earlier I mentioned the dangers of LDL or ‘bad cholesterol’. But there is also ‘good cholesterol’ otherwise called high density lipoproteins or HDL. And as you’ve probably guessed from the name, HDL is not dangerous to the artery wall like LDL because the particles are of a high density and are unable to squeeze in between the endothelial cells and deposit in the artery wall. In addition, HDL serves many benefits. HDL can reduce the inflammatory actions and the entry of macrophages into plaques while increasing their exit from atherosclerotic plaques, thus reducing the size of plaques even if they are already large in size. HDL also promotes the breakdown of cholesterol and its excretion by macrophages, thus reducing the fat content of plaques. So how can you increase your HDL levels? Foods that are known to increase HDL levels in the blood are: fish, high fibre foods (such as oats, fruit, vegetables, grains), nuts, legumes, yogurt, fruit juice, dark chocolate, garlic, and red wine (or dark grape juice if you don’t drink alcohol). And if you have been prescribed statins, keep taking them as they reduce LDL levels while increasing HDL in your blood, and have many anti-inflammatory benefits. 4) Don’t add salt to taste A high intake of salt increases blood pressure, and the higher your blood pressure the higher your risk of suffering a heart attack or stroke. A higher salt concentration in your blood promotes the diffusion of fluid; primarily water, into the circulation increasing blood volume and thus increasing pressure and potentially damaging the blood vessel wall, particularly the endothelial cells. When pulses of blood are pumped around the body, the arteries need to expand and relax with each pulse of blood that moves through. But if the endothelial cells are damaged, they cannot send signals to stimulate the expansion of the vessel wall further increasing the pressure created by flowing blood and imposing stress on the cells. All of these events increase inflammation creating the conditions for atherosclerosis to begin and further increase blood pressure.  You can have just one! You can have just one! 5) Don’t give in to your sweet tooth There is no doubt about the association between high sugar intake and cardiovascular disease, but we still don’t really know why this is the case. Studies performed so far suggest that high blood glucose levels can increase inflammation, promote the entry of macrophages into the artery wall and possibly interfere with the expulsion of cholesterol by macrophages. It also appears that LDL is increased in diabetics, thus sugar and cholesterol may work together to promote atherosclerosis. While more studies are needed to firm up these conclusions, the link between diabetes and cardiovascular disease is very clear so don’t tickle you sweet tooth too often! 6) Limit the booze Early studies demonstrate that light drinking (up to the recommended 2-3 units of alcohol a day) reduces atherosclerosis, and the risk of strokes and heart attacks, but consuming higher amounts of alcohol on a regular basis increases atherosclerosis significantly. But a recent small-scale study published by New Scientist [1] showed that when regular social drinkers gave up alcohol for a month, they experienced a large drop in liver fat, blood glucose and cholesterol, and improved their sleep quality and concentration, although more scientific evidence is needed to back up these results. So you can still enjoy that tipple, but only in moderation. [1]http://www.newscientist.com/article/mg22129502.600-our-liver-vacation-is-a-dry-january-really-worth-it.html?full=true#.U5MZJxblk2w Any questions? Please comment below Ten years ago when my father was hospitalised after suffering a heart attack, the nurses gave him a video to watch about heart attacks. The video detailed the symptoms and treatment given, and when addressing the cause of heart attacks, the narrator stated that it is not really known, all is known is that a blood clot arises blocking the artery’s blood flow from reaching the heart, thus starving the heart muscle of vital nutrients and oxygen for survival and ultimately damaging the heart. While the latter is true, the events prior to blood clot formation have been well known for years, in fact centuries! A more accurate statement would have been that it is not fully understood how the various symptoms of a heart attack, such as vomiting and excessive sweating, occur. Nonetheless as an A-level student, this deepened my curiosity into the cause of heart attacks ultimately leading me to undertake a PhD on atherosclerosis – which I will define later in this post. If you watched the second episode of the recent “Watermen: A Dirty Business” series on BBC Two, you will have seen how drains are often blocked because hundreds of litres of cooking fat is poured down household sinks every week. Over time the fat builds up inside the pipework, particularly at joints and bends, eventually blocking the pipes and causing the rather unpleasant consequence of sewage spewing out onto the roads! The process of fat blocking our sewage pipes is reminiscent of what happens in our own arteries.  Sewage pipes - Looks just like a clogged artery doesn't it? Urgh! Image from www.dec.ny.gov So what is the disease inside our arteries that can have such deadly consequences? Firstly it is important to clear up a couple of terms which can cause confusion, even to me! Arteriosclerosis refers to the hardening and thickening of the arterial walls. The middle layer of the artery wall (the tunica media) primarily consists of smooth muscle cells, which contract and relax, like our muscles, to create an elastic effect so that each time the heart pumps, the artery wall expands and constricts to allow pulses of blood to flow through. Hardening of the artery wall means this elasticity is lost and blood pressure increases in the artery. The subsequent narrowing of the artery reduces the ability of blood to flow to the intended tissues. Hardening can occur for several reasons; calcium deposits can build up in the tunica media. Or a process called intimal hyperplasia can occur (please don’t worry too much about the jargon!) where smooth muscle cells multiply excessively and move towards the inner layer of the artery wall. ‘Intimal’ refers to the innermost layer of the artery – the intima, and ‘hyperplasia’ refers to the excess reproduction or multiplication of cells. Additionally the smooth muscle cells produce proteins such as collagen and elastic fibres further hardening and clogging up the artery. But the main type of arteriosclerosis causing major problems in the human population, and primarily responsible for heart attacks and strokes, is atherosclerosis. It is a disease that takes decades to develop and inflict its potent consequences on us but by the time we know it’s happening, it is often too late. So what exactly is atherosclerosis? As you read the next part, watch this video which may help you visualise the disease (video created by 3FX medical animation inc.): Just like the fatty sewage pipes, atherosclerosis begins at bends and branches of arteries. Blood pressure can be high in these regions, and the blood tends to slow down or swirl around causing the cells lining the inside of the artery (called endothelial cells) to become ‘activated’ setting off a chain of events. Firstly ‘lipids’ including cholesterol – particularly low density lipoproteins, more commonly known as ‘bad cholesterol’ - deposit in the artery wall in between the endothelial cells; hence why you should stay away from those pesky fast food outlets! But atherosclerosis is not simply a fatty plaque that blocks your artery. As these lipids slowly build up in the artery, our immune system is called to action by the active endothelial cells and sends in cells called macrophages to consume, break down and dispose of these lipids, and initially they are successful. But over time the amount of lipid building up can become excessive and overwhelm the macrophages, so these cells consume surplus lipid and become immobile, just like if you eat too much chocolate cake and feel so sick you can’t move! The macrophages eventually die and add to the material building up in the artery wall. There are many other types of immune cell that become involved and contribute to the problem but macrophages are the main protagonist (and incidentally the main cell of interest in my research!) The artery tries to tackle this problem by expanding outwards to increase the diameter of the artery, and by moving smooth muscle cells from the wall to the surface of what is now a developing atherosclerotic plaque. The smooth muscle cells create a ‘cap’ at the surface separating blood flow from the plaque as exposure of dead cells to flowing blood can trigger the formation of a blood clot. Eventually the artery cannot expand any further and so the growing plaque begins to constrict blood flow. The growing plaque can be enough to obstruct blood flow. Narrowing of the artery also causes the flowing blood to exert force on the cap and weaken it eventually causing it to burst open or rupture. A blood clot will then form on the surface, which may or may not block blood flow in the artery. If blood flow is blocked in the coronary arteries supplying blood to heart muscle, a heart attack occurs and some of the heart muscle can die. Alternatively blocking blood flow to part of the brain, either by a blood clot or part of a plaque dislodging and blocking the small blood vessels in the brain, leads to a stroke. So atherosclerosis is an extremely complex process with many different factors involved, hence why it is so difficult to treat. Research is vital to fully understand this disease and improve existing treatments. Much like cancer, which is so difficult to treat because cancer in each patient can be caused by a different mutation in a different gene, thus we cannot use a ‘one size fits all’ drug. Now that you know what atherosclerosis is, I will explore how you can reduce your risk of suffering from a heart attack or stroke in my next post. |
AuthorDr. Anusha Seneviratne  This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. 
Categories
All
Archives
March 2020
|

