PART 4: PRIORITISING PLANETARY HEALTH Today many health policy analyses recognise the health issues occurring in response to climate change, such as the spread of tropical diseases and human migration due to the detrimental effect on resources. Health organisations seek to develop healthcare systems to cope with increasing demands that will emanate due to worsening climate change. However, as we have seen in the last three posts, there are many man-made issues that are causing both serious human health and environmental issues simultaneously and thus contributing to climate change. Nature has an abundance of complex mechanisms to deal with any challenge from pest control to natural disasters, but human manipulation of these systems has had a detrimental effect on our environment and is having a knock-on effect on us and threatening humanity’s future. We have already learnt so much from nature from discovering medicines to building aircraft inspired by the aerodynamics of bird flight. We must continue to learn from nature to find solutions for our planet’s future.  Don't you want to be surrounded by this all the time? Photo credit: adiceles | Pxhere PART 3: THE ECOLOGICAL CRISIS In part 2, I explored how our desire for foods or substances that are detrimental to our health in excess, is leading to extensive environmental damage due to large scale manufacturing and waste. In this part, I will examine factors that have been well known to damage our environment for some time and explore how these factors are also damaging our well-being more directly than we think.  Rising rates of deforestation is diminishing our ability to tackle climate change. Save our trees
One of the first scientific concepts we learn in school is photosynthesis - the conversion of sunlight and carbon dioxide in the air into oxygen, by green chlorophyll contained in chloroplasts in the leaves of plants and trees. Oxygen is the very gas that is necessary for us to live. Combined with glucose it fuels every single cell in our bodies. Without it, we will die - it cannot be emphasised enough! And yet when housing is built, more land is needed for agriculture, or precious metals are mined, trees are swept aside as if they are a mere obstruction, often illegally. It is estimated we have lost more than half of the planet's tree cover since humans came into existence [1]. Currently in England, we are battling the prospect of the HS2 high speed railway line, which despite not yet having the official go-ahead, has already caused the clearance of green areas, with many more ancient woodlands under threat, some of which are hundreds of years old. Such ancient trees support rare wildlife species and ecosystems that are so complex, we still don't fully understand them. While this has so far had a negligible effect on atmospheric oxygen due to production from other sources such as oceanic plankton, it is only a matter time before the balance tips over the edge. PART 2: OVERCONSUMPTION VS PLANETARY HEALTH In part 1, I examined the most potent sources of man-made pollution and their effects on the environment, wildlife and human health. In this part, I will explore how certain substances we consume in excess can not only damage our health and human rights, but also means huge swathes of land is lost for nature.  Sugar cane plantations like this one in Karnataka, India, are fast eating up land where native forests lie. Photo credit: pxhere.com Sugar
Increasing levels of sugar in our food has become a great concern among health professionals as rates of diabetes, obesity - particularly among children - and heart disease are on the rise in the developed world, and are rapidly rising among younger people in the developing world, as we increasingly indulge in sweets, cakes and fizzy drinks. In one of my previous blog posts, I discussed how excess sugar can increase the risk of vascular disease and subsequently heart attacks and strokes [1]. On a personal level, I am often frustrated by the levels of sugar present in food items in the supermarket and with diabetes in my family, I am puzzled by how diabetics can control their blood sugar levels as sugar is even added to foods that should be savoury. Of course, we shouldn't eliminate sugar from our diets as it provides vital energy for our cells, but the levels added to many foods are excessive and unnecessary. Measures are being put in place to crack down on the food industry's indulgence in sugar, such as the sugar tax that was implemented in the UK in 2018. PART 1: POLLUTING THE PLANET  Free-Photos at Pixabay As I read about the environmental destruction carried out by multi-national corporations clearing land to grow palm oil, sugar cane and other crops in the book "Landgrabbers" by Fred Pearce, I learned how we are producing foodstuffs and other materials at an unnecessarily large scale to satisfy a human population accustomed to consumerism. While poorer populations who lived in harmony with nature for thousands of years, have their human rights neglected and even lose their lives. Consumerism is driving behaviour that eventually harms the long-term health and welfare of humanity. Increasing urbanisation and economic development means our lives are more absorbed with gaining wealth, keeping up with the latest trends and a throwaway culture. In addition, human overpopulation is increasing competition for limited resources, adding to the anti-immigrant sentiment felt in many countries.
I thought the brilliant "People's Manifesto for Wildlife" initiated by Chris Packham in 2018 could be strengthened by including a Ministry for the environment and human health. As I searched online for existing policies, the most common policy area I encountered was the effect of climate change on human health and how to develop more resilient health systems. It seems not many were making the connection that many causes of environmental damage, climate change and the ecological crisis, are also causes of many human diseases and have detrimental effects on quality of life. It is only in the last few years health policy experts introduced the concept of ‘Planetary Health’, defined as “the health of human civilisation and the state of the natural systems on which it depends” [1,2]. While there is increased awareness of Earth's dire situation over the last couple of years, making the necessary changes happen fast is proving a challenge with the recent surge of right-wing anti-environmentalism reaching powerful positions in the form of the current US and Brazilian Presidents for example. We have a lot of work to do in very little time. Before we tackle the awkward question of overpopulation, we can have a massive impact by discouraging consumerism and developing existing technologies to cut carbon emissions. Many believe meaningful change means a poorer quality of life, which has some truth as developed countries are responsible for far more carbon emissions than developing nations. But is that a reasonable association to make? Some indulgences must be stopped but is that such a bad thing for our welfare? I hope my next four blog posts will offer a different perspective and a deeper understanding of how we depend on the natural world to survive, and why we need to save it fast. In this series, I will examine how solutions for our planetary crisis will benefit our quality of life and health. And how it won't necessarily come with the cost of living poorer lives. I will explore the common causes of non-communicable diseases and loss of land for nature, and why thriving natural ecosystems are essential for our well-being. But first, I will look at some of the sources of pollution that are damaging our ecosystems and our health.  I am excited to share that as a result of my previous blog post "Can infection cause chronic disease?", I was invited by the World Health Organization's (WHO) Non-Communicable Diseases office to contribute to a WHO report on Men's Health in the European Region!
The report is a comprehensive analysis of the various health challenges men face, the current state of health systems underpinning those issues, and provides proposals on further research and the policy changes necessary to improve the outlook for men's health in Europe. If you would like to read this report, go to the link below, and you will see my name in the acknowledgements page. www.euro.who.int/__data/assets/pdf_file/0007/380716/mhr-report-eng.pdf?ua=1 I would like to thank Dr. Kremlin Wickramasinghe at the WHO for this opportunity, and I hope this report will have a far reaching impact in health policy. 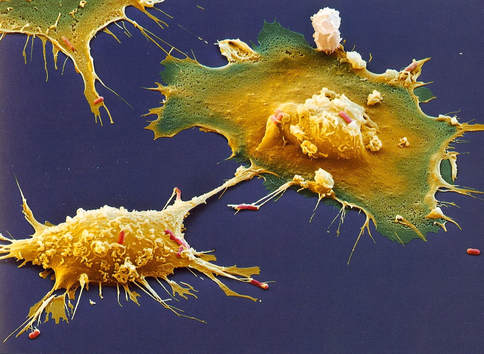
Macrophages detect infection but also exacerbate atherosclerosis. Therefore could infection indirectly cause atherosclerosis and other chronic diseases?
Update: An edited version of this article has been published by Antibody Genie. Thanks to Dr. Colm Ryan for the invitation. Check out the article here: www.antibodygenie.com/blog/can-infection-cause-chronic-disease/
With non-communicable diseases (or NCDs, which include heart disease, diabetes, cancer) now responsible for the most deaths worldwide, large investments into research on these diseases are helping us understand their causes. Many of these diseases have something in common, they involve chronic inflammation. Cells normally triggered by the immune system to fight infection, are persistently activated by factors produced within the body (endogenous factors), eventually causing damage to bodily tissues and beginning the disease processes involved in the development of diabetes, cancer and atherosclerosis - the build-up of fatty plaques in the arteries causing heart attacks and strokes. This begs the question, if both infection and endogenous factors can trigger the same immune responses that are known to cause NCDs, could infection directly cause NCDs?
Triggering our immune defences A good example of the responses triggered by both infection and endogenous factors starts with the well-characterised family of Toll-like receptors (TLRs), which are found on the surface of many immune cells. These receptors play a key role in innate immunity – the first line of defence against infection. Each of the 9 members of the TLR family recognise different components of pathogens, for example TLR4 recognises lipopolysaccharide (LPS) found on the outer membrane of certain types of bacteria, and TLRs 3 and 7 recognise viral ribonucleic acids or RNAs, which viruses release into the host cell they infect to exploit the cell’s machinery to produce its damaging viral proteins. When TLRs bind to a molecule they recognise, they can activate a sequence of proteins ending with a protein called NFkB (NFkappaB) and/or the Interferon regulatory factor (IRF) family, which are responsible for the production of numerous inflammatory proteins [1]. Once an immune response is triggered following TLR activation, it is usually sufficient to successfully destroy the infection. Thus, the infection is short-lived and the immune system can return to a resting state. 
Your cells die every day. Don’t worry, your body is protecting itself. In a process known as apoptosis or programmed cell death, cells that are no longer needed commit suicide. Some cells are only required for a short time, they maybe infected by a virus or develop harmful cancerous mutations. Cell death is also an essential part of development from an embryo. For example mouse paws begin as spade-like structures and only form the individual digits as the cells in between die [1]. During apoptosis the cells fragment into smaller apoptotic bodies, and their cell surface is flipped open to display lipid molecules called phosphatidylserines, which act as an “eat me” signal to recruit cells called macrophages to engulf them, before their contents spill out and damage the surrounding tissue. This is a process known as efferocytosis.
However cell death is not always so orderly. Some cells suffer premature death known as necrosis, where they burst open for various reasons such as infection, physical trauma or extreme temperatures. However as the cell’s contents are released into the open, an inflammatory response is triggered, so the macrophages sent to engulf these cells release substances that can damage the surrounding tissue, resulting in a build-up of dead cells. It is this damaging chain of events that often occurs in atherosclerosis; the build-up of fatty plaques which can block arteries or trigger blood clots leading to heart attacks, strokes or tissue death, known as ischaemia. As fatty lipid molecules (primarily LDL or ‘bad’ cholesterol) build up in arteries, they act like damage signals. Macrophages recognise these damage signals as if it is phosphatidylserine, and engulf the lipids to become what is known as a foam cell; a cell full of lipid. A healthy macrophage can repackage the LDL into larger HDL cholesterol, which is released back into the bloodstream to be excreted by the liver. The foam cell can also leave the atherosclerotic plaque to be disposed of via lymphatic vessels, thus shrinking the plaque. However, foam cells can be overwhelmed by engulfing excess cholesterol, increasing harmful inflammatory signals, stress and apoptosis. But all is not lost here. If other macrophages clear the dying foam cells, less harm will be done. The problem is the increased inflammation renders efferocytosis defective, resulting in a process called secondary necrosis. Here apoptotic bodies swell and burst open, as they haven’t been cleared in time. As a result, a large amount of cell debris builds up inside the atherosclerotic plaque, creating what is referred to as a necrotic core. The core is pro-thrombotic when it is exposed to clotting factors in the bloodstream.  Protestors outside the Hammersmith hospital demonstrating against the closure of its A&E unit in 2014. Photo credit: @AnushaNS December 12th 2014 was declared Universal Health Coverage (UHC) Day worldwide as 587 academic institutions, non-governmental organisations and health charities campaigned for healthcare to be universally available so that epidemics such as Ebola, Malaria and Heart Disease can be tackled, particularly in developing countries. This movement has been inspired by successful healthcare systems in developed countries, which have improved the health of their populations while also boosting their own economies as a result of a healthier workforce. One such paradigm is the UK’s National Health Service (NHS). Founded in 1948 by the Labour party, it is now the largest publicly funded health service in the world, and was recently rated the best health service amongst 12 developed countries.
Since the Health and Social Care Act was passed by the Conservative and Liberal Democrat coalition government in 2012, there has been increasing concern that the NHS will not be a ‘free-for-all’ health service for much longer. We have already witnessed nurses losing their jobs, hospital A&E wards being shut down and surgical procedures being curbed in an effort to meet the government’s demand of £20 billion in savings by this year. It is no wonder, as the NHS actually requires another £30 billion each year to stay afloat by 2020. A study in the British Medical Journal last year showed that private sector providers secured 33% of NHS contracts in the preceding 12-month period [2]. It was even discussed that GP consultations should require a £10 charge, although the British Medical Association rejected this motion. It seems profit will become and increasingly influential factor in the provision of health services in the years to come, thus the NHS may struggle to maintain its status as the gold standard for the provision of healthcare worldwide. This is perhaps driven by an American-style mentality where any socialist system is feared as an attempt by government to control the population. As NHS services are slowly eroded, so too will the health of the UK population, the ability of the UK to remain a world leader in medical innovation, and the strength of Britain’s economy. So what if the NHS became inaccessible or unaffordable to the poorest in Britain? We have seen the havoc created by private insurance companies in the US and elsewhere, who often reject ‘high-risk’ patients deeming them too costly. Hence the poorest and most vulnerable in society cannot afford healthcare they so desperately need. However other patients are not safe either. Deceitful persons can exploit them due to their lack of medical knowledge. This scenario has been particularly evident in the Indian states of Madhya Pradesh and Uttar Pradesh, where an inefficient healthcare system has allowed exploitative companies to run riot [3]. Let’s take a look at how universal healthcare has benefited developing countries. There are many examples where good basic healthcare has been provided at a very low cost. In 2001, Thailand introduced a nationwide system where no patient would have to pay more than 60p per visit for medical care, while the poorest quarter of the population were exempt from charges [3]. As a result mortality rates, particularly in children, have fallen while life expectancy has risen significantly. The new Thai health system has also demonstrated that with widely available preventative care and early intervention, the need for expensive treatments and surgical procedures has plummeted. Readily available healthcare is also essential to fight infectious disease epidemics, should one ever arise in the UK. We have seen in Western Africa that if countries surrounding Guinea, where the most recent Ebola outbreak began, had effective universal healthcare systems, this could have alleviated the outbreak or even prevented Ebola from spreading throughout the region. This is why Nigel Farage’s shameful comment on HIV diagnoses in the recent seven party election debate was so short-sighted, in addition to being entirely false. If we were to reject treatment for HIV patients born overseas, we would be leaving the door ajar for HIV to be readily transmitted within the UK population as well as in surrounding countries, facilitating what is already a global pandemic. There is no doubt that social inequality needs to be addressed to tackle some of the country’s major health burdens, something the major political parties seem unwilling to confront. The poorest in society are more vulnerable to harmful behaviours such as smoking, abuse of alcohol and drugs, and mental health problems. Anxiety and chronic stress caused by redundancy and poverty can weaken the immune system and increase risk of cancer and cardiovascular disease. But a strong universal healthcare system plays a large role in tackling inequality, while benefiting the economy. This has been evident in the once comparatively poor Indian state of Kerala, where universal healthcare and schooling has helped the state achieve the highest per capita income among all Indian states [3]. Cuba has been subject to US sanctions for several decades, but it has one of the highest doctor to patient ratios and vaccination rates in the world, and life expectancies are similar to the US population. Cuba is even able to offer help to other countries by flying out doctors to scenes of natural and humanitarian disasters. The Lancet recently published a proposed manifesto to improve five key areas in the NHS [4]: · The currently poor interface between general practice and A&E medicine. · The modest way child and adolescent health care is delivered. · End the false dichotomy between mental and physical health. · Stop neglecting early diagnosis and prevention. · Act on elderly and social care. It has also been argued that other measures need to be taken to make GPs more accessible such as extending GP opening hours, and making appointments available online and by phone [5]. I have already explored how the NHS is vital for the UK to maintain its status as one of the greatest medical innovators in the world [6]. Such innovation is essential to tackle major problems of the future such as the prevalence of antibiotic resistance and treating the ageing population who often suffer from a multitude of conditions requiring careful management. Innovations include the development of genomic medicine and healthcare technologies such as wearable devices and smartphones. In the last five years, the current government has frozen research budgets, resulting in a net loss of funding due to inflation. There is an emphasis on investing in the ‘Golden Triangle’ of London, Oxford and Cambridge, which needs to end. Investing in other parts of the country would not only benefit science, but also health, economic and social regeneration [4]. We also need the NHS to train our future doctors and innovators. However this has been compounded by the recent hike in tuition fees, resulting in fewer applications to university among A-level students. Climate change is also a major threat to the health of the global population. Insect-borne diseases could come closer to home, extreme heat can kill those with existing heart and lung problems, pollutants can increase the risk of lung cancer heart disease, and the loss of homes and livelihoods due to floods or droughts can cause depression [7]. Such a threat requires action on a global scale. While it is encouraging that the UK has increased its international development budget to 0.7% of GDP, more advocacy work is required by the UK to act as a leader in advancing universal healthcare globally [4]. So as we reach the final month before the UK’s general election, who can we trust to bring about the changes the NHS needs? We have already witnessed how the current coalition government, headed by the Conservatives, have introduced a culture of austerity and privatisation that has sent pulses racing among ordinary citizens. The results of more encouraging measures, such as a pilot scheme where opening hours in 14% of GP practices were extended, are yet to be seen. In their election manifesto, the Labour party have pledged to recruit 8,000 more GPs and guarantee an appointment within 48 hours. This maybe a far reaching goal as the largest increase in the number of GPs in any parliamentary term in the last 20 years was 5,414, while the last Labour government was only able to deliver their guarantee of an appointment within 48 hours to 81% of patients [5]. However their pledges are a step forward, and could be better than anything we could ever hope for from another five years of Conservative leadership. References [1] http://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirror-mirror [2] http://www.nationalhealthexecutive.com/News/nhs-facing-creeping-privatisation- [3]http://www.theguardian.com/society/2015/jan/06/-sp-universal-healthcare-the-affordable-dream-amartya-sen [4] http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2815%2960467-6/fulltext [5] http://www.bmj.com/content/350/bmj.h1513 [6] https://www.the-newshub.com/uk-politics/why-the-nhs-is-vital-for-the-future-of-medicine [7] http://www.newscientist.com/special/NHS 
British Prime Minister David Cameron recently announced that those individuals, who refuse treatment for their obesity, alcohol or drug problems, could have their sickness benefits cut. Such a statement appears to stem from a view that these individuals intentionally neglect themselves, and that punishing them will deter such behaviour in the future. The reality is very different.
We all know that obesity is the result of excess consumption of foods with a high content of sugar, salt and fat. Alcohol and drug addiction are often due to an individual’s desire to seek comfort and relief, perhaps to escape from difficult personal circumstances such as redundancy or losing a loved one. But it is the introduction to these foods and substances that is the real issue, and what is responsible for this? Advertising. In the Western world, and now becoming increasingly common in developing countries, we are bombarded by billboard, television and newspaper adverts for all types of fast food burgers, alluring chocolates and “invigorating” tipples. You probably haven’t realised this as you go about your everyday life. Have you ever walked past a patisserie window without wanting to stuff your face with cake? Children are particularly prone to giving in to such advertising. If you give in to your senses and devour such unwholesome grub, you will be left wanting more. In fact, excess sugar and salt intake, in addition to alcohol and drug consumption, increase the activity of dopamine neural pathways in the brain, commonly viewed as a reward circuit in the brain. With this level of temptation surrounding us, it is no wonder that some individuals fall victim to a vicious cycle of cravings and bingeing, much like the addictive behaviour observed in alcoholics and drug addicts. In addition, the low cost of fast food makes it a more affordable option than healthier alternatives, for those who maybe struggling with their finances. There also lies a cultural problem, particularly with regards to alcohol consumption. Alcohol is widely seen as an essential ingredient to engage socially, by abandoning one’s inhibitions and leaving behind the woes of life. Coercion from peers can often lead to one consuming alcohol when they are otherwise trying to abstain, or risk being excluded from the social circle all together. Moreover advertising by alcohol brands glamorizes beverages with the use of celebrity endorsements and images of partying hard. While many do drink responsibly in social environments, binge drinking is on the rise - which has been proven to have detrimental health effects such as brain damage in teenagers, and muting one’s immune responses to infection. And if an individual were to unexpectedly face difficult personal circumstances, they could see alcohol as a source of refuge – due to its ‘positive’ image - and attempt to drown their sorrows. The fact is alcohol will only provide temporary respite from such problems. It is not the solution, and so the despair deepens. When we consider all of these points, it is clear that people suffering from addictions need help, punishing them by withdrawing their benefits is not productive in the slightest. It will only send them into deeper despair, exacerbating their harmful behaviours. These patients require strong psychological support from the health service as well as those closest to them. We must also bear in mind that these patients may be suffering from other health problems that could be causing or complicating their health, preventing them from working and exercising, such as diabetes, arthritis or accidental injuries. In these circumstances, it is highly unlikely that obese individuals will refuse treatment. These patients require careful and rigorous management of their health, of which only qualified health professionals can provide. This debate underlines the argument that good health is a human right. An individual’s personal choices and financial circumstances should not be detrimental to their health, especially when the environment surrounding them heavily influences such choices. Providing the best support possible for these patients can only be beneficial for the country, by potentially allowing them to return to work and contribute to the UK economy. On the other hand an oppressive approach, coupled with the reduction in quality and quantity of NHS services is neither beneficial for patients or the economy. This piece was written for The News Hub. Please visit https://www.the-newshub.com/health-and-fitness/punishment-is-not-the-answer-to-health-problems and give it a vote up! Lessons from the Standing Up for Science Media Workshop in london organised by Sense About Science  Do you know what the following claims have in common?
I hope you have realised that none of these claims have any substantial evidence to support them, so we can safely assume they are false [1,2]. Everyday we are bombarded by adverts and stories in the news detailing the latest scientific advances and companies selling their newest health and beauty products. How can us scientists ensure the wrong information does not reach the public? The mainstream media is often criticised for biased reporting of current affairs. They have also angered many scientists for dumbing down the science when reporting about newly published studies, or even distorting the main findings to support one’s agenda, perhaps politically motivated. Quite unexpectedly tabloid newspapers can be more accurate at reporting science stories than broadsheet newspapers. While hyping up a study, as “the next miracle cure for cancer” will undoubtedly garner attention and increase newspaper sales, their intentions are not always so covetous. Newsrooms are incredibly competitive environments, so the pressure to release an attractive story can be so immense that erroneous reporting can slip through. Journalists actually do welcome help to interpret the latest studies, after all they are not trained scientists, so how can we expect them to critically analyse data from a study like a trained scientist can! And it is incredibly damaging for a journalist in the long term if they become known for misreporting a study, as scientists will not trust them if they receive a request for interview. Journalists often use #journorequest on Twitter to find experts to help them on a story. How can you ensure the main message of your study doesn’t get lost in the media hype? If your study gains massive media attention, be prepared for interviews, and have three clear messages that you can repeat. Learn to speak in repeated sound bites, as you generally do not have much time to have your say. As you are the expert of the study, be prepared to engage with people with all levels of intellect. If you believe your study is not receiving the attention it deserves, then get your word out there. Practice writing about your study in a short but interpretable manner, as if it were a newspaper headline. Even try writing and circulating press releases to get yourself known and trusted in the media as an expert in your field of research. When writing your press release, target it towards a journalist specialising in scientific reporting. It also pays to go to your university press office and talk about your research; they like to hear from active researchers. However it is interesting to note that journalists do not always trust university press releases, as they have been known to exaggerate the impact of a study, due to their reliance on publicity to obtain further funding. The terminology you use is extremely important, as words can have different meanings in different disciplines. For example the word ‘significance’ to a scientist means that the p-value obtained from a statistical analysis is small enough that the null hypothesis can be rejected. For example a treatment is shown to significantly reduce cell death in comparison to administering water, the null hypothesis in this case would be that the treatment does not affect cell death. But to the general public or a journalist, significance means something that is important and worthy of attention. So to relay your message, it is important to use simpler and understandable terms, and speak in the journalist’s language. This does not necessarily mean dumbing down the science; you just need to disseminate the core message. You cannot expect the public as non-scientists to understand all of the hard-core science. So there is plenty a scientist can do to help the media report science accurately. But as a member of the public, what can you actually believe? If you see an advertisement or news story and you are not quite sure if there is any evidence to back it up, there is something you can do about it – ask for evidence! Sense About Science has launched a brand new website: www.askforevidence.org, which gives guidance on how you can ask for evidence. You can directly email the company/journalist/publication and request to see evidence behind the claim, or you can fill in a form on the Ask For Evidence website. Companies have already been forced to withdraw products or advertisements, and change policies as a result of being asked for evidence they could not provide to support their claims. Sense About Science also regularly teams up with scientists in the Voice of Young Science network to examine the evidence behind suspicious claims, for example the use of homeopathy in developing countries, and the promotion of detox diets and products. You can see more about their campaigns here: http://www.senseaboutscience.org/pages/voys-campaigns-64.html. So put your critical thinking hat on and ask for evidence the next time you see something a little dodgy. The more people ask for evidence, the more people will expect to be asked, thus we can create a huge culture change. References [1] Book by Ben Goldacre (2009) Bad Science, Harper Perennial, UK. [2] http://www.senseaboutscience.org/pages/homeopathy-in-developing-countries.html |
AuthorDr. Anusha Seneviratne  This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. 
Categories
All
Archives
March 2020
|
